


Want to bend the curve? Abolish police and prisons
Prisons and jails were a public health crisis before the pandemic. In the middle of one, they're an engine for mass producing infection

This is the first of a short series of posts looking at a few institutions in America and how their current operations limit our fundamental ability to hold the pandemic at bay. This will likely be a set of three posts: today’s is on prisons, jails, and our carceral system more broadly; and following posts will look at schools and nursing homes (I’ll add links to these as they’re finished). Each of these institutions is usually talked about in the context of risk of infection within the institution itself, as though each were a discrete, walled garden. (Or, to use an unbearably on the nose academic reference, an ironic literalization of Foucault’s idea of the “carceral archipelago”). Instead it’s important to understand these institutions as drivers of the pandemic; each a machine for producing new infections.

[Image description: woodcut depicting “the eye of God,” 1551]
There are subtler ways of killing. Call it death by statistics. Today, white man lets his statistics do the killing for him. … Those statistics amount to genocide. Genocide also disguises itself in the form of poor health facilities and wretched housing and inadequate schooling and rampant corruption. ”
—Leonard Peltier, in “Prison Writings”
That prisons and jails are the sites of near-constant atrocity is an open secret. It lives underneath the veneer of every facet of liberal society, from our entertainment to the language we use to understand discipline and consequence. Prisons and jails institutionalize so many forms of direct violence and exploitation that it is almost possible to neglect what they do in ways that are indirect. I’ve quoted from Leonard Peltier above because I recall his writing as my first exposure to how withheld or improper medical treatment within prisons does violence to the incarcerated. Reading his accounts of systemic neglect infuriated me as a teen in 1999; that he and others face the same violence still, some twenty years later, is unconscionable.
For most of this post I want to focus on how prisons and jails are operating under the pandemic, and how they are actively fueling the spread of new infections both within and without. Suffice it to say that even prior to the pandemic the conditions the United States holds incarcerated people in were actively killing people. Last fall, migrant detention centers started to see mumps cases, a disease we’ve had a vaccine for since 1967 that was nearly eradicated within the U.S. Studies have estimated that incarcerated individuals’ physiological age averages 10 to 15 years older than their chronological age. Poor conditions in prisons and jails profoundly impact people with underlying medical conditions, particularly the disabled, who make up a disproportionate amount of the incarcerated.
As I’ve touched on previously, the outset of the pandemic has only exacerbated these conditions. To a viral infection, prisons and jails are what one attorney rightly called a “tinder box.” This is a darkly efficient metaphor, as tinder is consumed in the service of creating a larger fire.
A study was released in Health Affairs in June on incarceration and the coronavirus that looked at precisely this, and I highly recommend reading it in full to see the breadth of its implications, though I’ll cite it extensively below. (We also spoke about it on an episode of Death Panel in June). Looking at infection data from Illinois through April 19th, the authors suggest that jail cycling through Cook County Jail in Chicago—a single jail—was associated with 15.7% of new coronavirus infections in the entire state of Illinois, and 15.9% of new cases in the city of Chicago. In the words of the authors:
Our research evaluates how, following arrest and subsequent cycling in and out of jails as individuals await hearings and trials, the infection risk to those processed through the jail system may multiply into a generalized risk to the public. … as arrested individuals are exposed to high-risk spaces for infection in jails and then later released to their communities, the criminal justice system is turning them into potential disease vectors for their families, neighbors, and, ultimately, the general public.
They break this down by analyzing rates of coronavirus cases by zip code, finding that communities that are subject to more jail cycling (zip codes where arrests are more prevalent and the community is more policed) are by far a better predictor for a greater amount of cases than any other indicator:
We find that jail cycling is a significant predictor of SARS-CoV-2 infection, accounting for 55 percent of the variance in case rates across zip codes in Chicago and 37 percent in Illinois. By comparison, jail cycling far exceeds race, poverty, public transit utilization, and population density as predictor of variance. [Emphasis added]
The important thing here is to remember that new cases, and the communities that face localized outbreaks, aren’t some predestined inevitability. To continue to cycle people in and out of a place like Cook County Jail, which experienced an early and terrible outbreak of COVID-19, can only be understood as a decision, where the consequences are systemically-induced infection and death. And this is a decision that is happening at scale, in part because people in positions of power have reacted to the months of civil unrest and calls for abolition either by diverting attention onto meager reforms or by blatant show of force. Meanwhile the weight of the crisis for incarcerated people remains on full view in media outlets and in public record: the New York Times’ coronavirus tracker shows that of major outbreak “clusters” in the United States 89 of the top 100 sites of outbreak are prisons, jails, or correctional facilities.
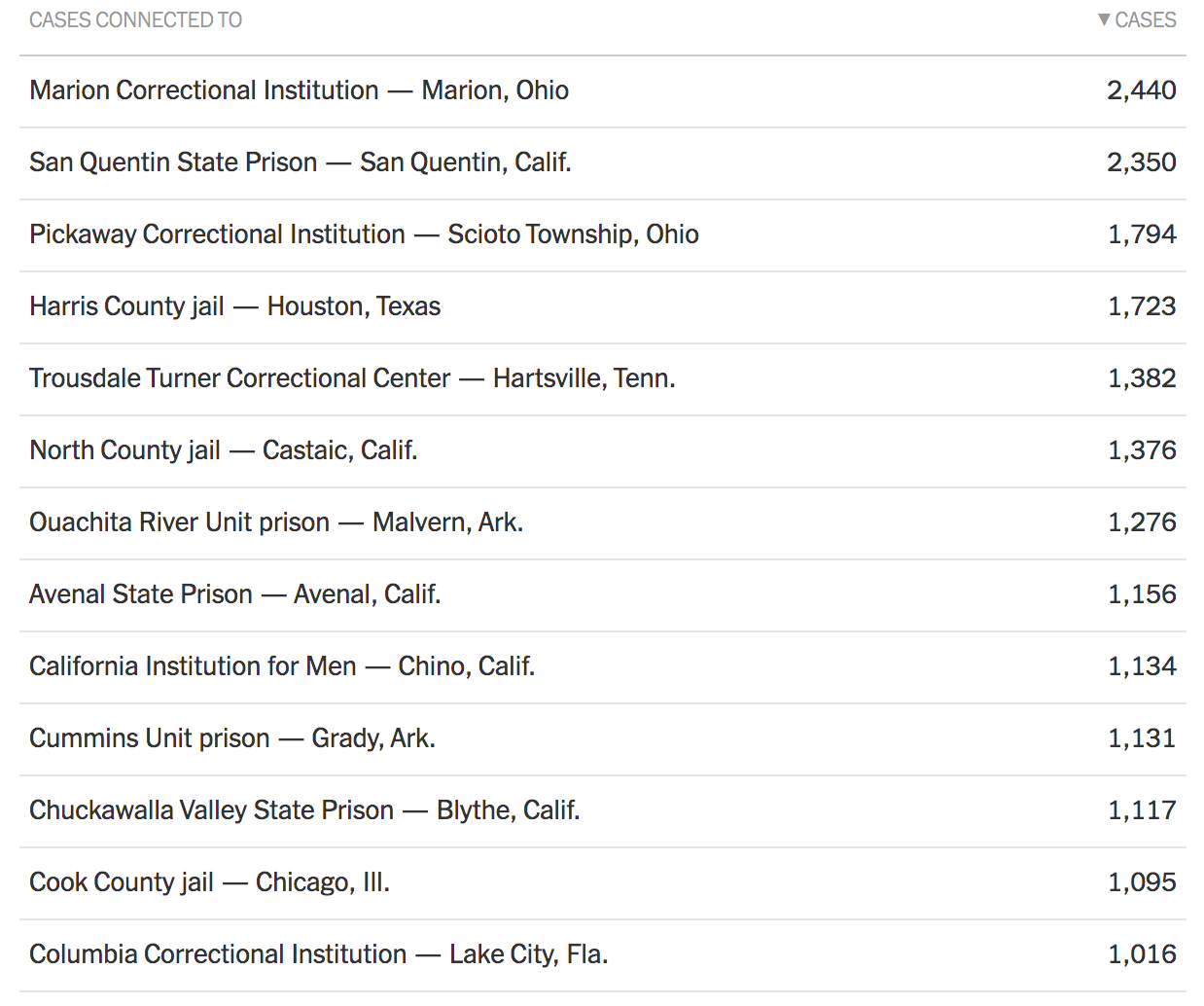
[Image description: Screenshot of New York Times coronavirus cases tracker. All listed in screenshot are prisons, jails, or correctional facilities.]
(Recall that the study on Cook County Jail is based on data up to April 19th; at that point Cook County Jail was only reporting between two and three hundred cases, a figure it has since surpassed).
To borrow from the Peltier quote above, these statistics amount to genocide. And this fact is even more evident when you consider that coronavirus spread in jails and prisons disproportionately harms the same people our carceral system already targets: Black, Indigenous, and people of color, trans and nonbinary people, and disabled people. In the case of Chicago, the study’s authors point out:
In light of the well-documented, disproportionate intensity of policing and incarceration in black neighborhoods in the United States, the carceral-community spread of disease may bear partial responsibility for the striking racial disparities noted in COVID-19 cases. In Chicago, although black residents comprise only 30 percent of the population, they represent 75 percent of the Cook County Jail population and 72 percent of the city’s COVID-19-related deaths.
To me this study presents solid evidence that white supremacy is a disease vector and the carceral system is its medium of transmission. This can’t be solved with miniscule reforms or building new jails to replace old ones. This can’t simply mean replacing cops with social workers, because as K Agbebiyi and others have argued, so much of the social worker profession is built around and within the carceral state.
Helpfully, on this point the study’s authors are explicit. They recommend changes to the carceral system and prison industrial complex (refreshing to see printed in Health Affairs), though stop short of employing the language of full abolition:
Our findings reinforce arguments that efforts to shift criminal justice administration away from arrest and incarceration may be vital for protecting the public health during this pandemic and reducing vulnerability to future epidemics. Waiting until epidemic outbreaks become apparent to implement changes in the criminal justice system, as in the present case, is not sufficient and will not protect against a reprise of the current situation.
But abolition is the only meaningful path forward. And it is an incredibly useful framework particularly because abolitionist thinkers recognize that prisons and policing are not components of an archipelago but features of a single mass. In a recent letter expanding on the 8 to Abolition project, K. Agbebiyi, Sarah T. Hamid, Rachel Kuo, and Mon Mohapatra write:
Police abolitionists have long been invested in dismantling pernicious and interlinked social systems: the prison industrial complex, the military-industrial complex, and the border. This is not just a politics of solidarity or co-liberation; these systems actively inform and condition policing in the United States. Police abolition must be anti-imperial and anti-militaristic—because American policing is co-constituted by practices of imperialism and militarization.
Dean Spade calls this “abolitionist discernment”: the ability to recognize what these systems share and how they reinforce one another. These are all sites of social subjugation that kill, maim, and devalue human lives to further the American imperialist project. They share legitimation strategies (Spade specifically names pinkwashing), tools and technologies, and they share tactics and a common language.
This kind of language should be familiar to anyone committed to health justice as well: the features we identify as the social determinants of health point to a need in our political economy that extends far past the reaches of enacting already-popular policies like Medicare for All. It’s a single mass. And it’s killing us.
Thank you for reading Health and Capital. As I mentioned in my introductory post, if you enjoyed this and would like to support my ability to produce future posts, please subscribe, share links to it, tell me what you think, and become a patron of the Death Panel on Patreon. Death Panel is a podcast I co-host with Beatrice Adler-Bolton, Philip Rocco, and Vince Patti, and if you enjoy Health and Capital you will probably enjoy it as well.
If you liked this post you may enjoy participating in the Death Panel’s community reading group on “Decarcerating Disability: Deinstitutionalization and Prison Abolition” by Liat Ben-Moshe, which happens on Sundays in our Discord server.


If you’d like to hear Beatrice’s interview with K Agbebiyi on a recent episode of Death Panel, the episode is embedded below.